Advice On Artificial Insemination For Sickle Cell
Hello Mirror Doctor, I have a little problem I want to seek advice from you. My fiancée and I are both sickle cell traits (AS). We have been to a doctor somewhere in Accra who said it can be eliminated from our children.
Once the baby is 16 weeks, there is a test to be done on the foetus to see if it has the sickle cell disease or just the trait. The other option is to go in for an artificial insemination with a donor sperm.
Please I need your help as I am very confused. What would be your advice?
Evelyn
Dear Evelyn, From your mail, you are both AS and so the chance of each pregnancy resulting in a foetus with sickle cell disease is 25%. This gives various combinations I believe the doctor you visited explained to you hence the suggested options to avoid sickle cell disease in the child.
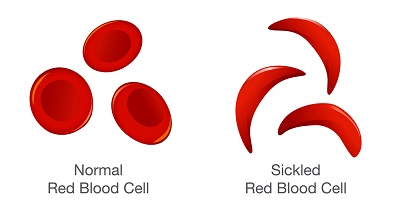
Why avoid giving birth to a child with sickle cell disease? Because of the complications associated with the condition. The underlying abnormality in sickle cell disease is that the red blood cells (RBC’s) are abnormally shaped.
This abnormality can result in serious infections, chronic anaemia and damage to body organs. Each person can have different forms of complications from the disorder. Some remain relatively stable, wManagement in children has focused on prevention of stressors that tip children into attacks or crisis. This can take different forms depending on which particular organ or system in the body is involved.
Most people with sickle cell disease have anaemia and may develop one or more of the following conditions and symptoms as part of the disorder:hile others are frequently hospitalised.
Acute chest syndrome – Inflammation or trapped red blood cells in the lungs.
Aplastic crisis – Bone marrow temporarily slows its production of RBC’s due to infection.
Hand-foot syndrome (dactylitis) – Painful swelling of the hands and feet.
Infection – People with sickle cell disease are at an increased risk for certain bacterial infections.
Painful crises – Can occur in any part of the body and may be caused by cold or dehydration. The pain may be so severe that hospitalisation would be required.
Splenic sequestration crises – The spleen becomes enlarged by trapping the abnormal RBC’s. This leads to fewer cells in the general circulation and worsens the anaemia with sometimes fatal consequences.
Stroke – Poor blood flow can occur in the brain when sickle cells block small blood vessels. This may lead to stroke.
Other possible complications can include leg ulcers, bone and joint damage, gallstones, kidney damage, painful prolonged erections in males, eye damage and delayed growth.
Besides bone marrow transplantation, there is no known cure for sickle cell disease. Transplant are complicated procedure and are not advised for everyone. To qualify the person would need bone marrow from a “matched” donor with low risk of rejection by the recipient.
Bone marrow transplant is currently in its infantile stages at the Accra Regional Hospital and even after transplant, the risk of transmission to the children still persists.
It is in light of these challenges that certain options are explored for couples who are both traits or one with the disease who have the desire to have children.
There is absolutely no problem if the couple decides not to have children but once they desire to have children, then the various combinations come in.
In your case, with each pregnancy, there is a 25% chance of the foetus being SS, 50% chance of being trait AS and 25% of having normal combinations of AA.
So, the technology of sampling the foetus at 16 weeks to determine if it has SS combinations is available. The more ethical dilemma which you both have to consider is what next in the event of the foetus coming as SS?
Are you both willing to have that foetus aborted? In addition, the sampling itself carries a small risk of losing the pregnancy, are you happy to go with that knowing that a foetus with normal combination or trait can be lost from complications of the procedure itself?
These are a few questions for you both to consider.
I am aware of technology in an assisted reproductive technique where before the embryo is implanted, a portion is sent for analysis to determine the genotype to prevent giving birth to a child with sickle cell disease.
I’m not sure if this technology is available in Ghana and it has a huge cost implications in addition to the failure rate of these assisted reproductive techniques. This is also something to consider.
The final consideration from your mail is to use the sperm or egg of a donor, Again, this is something to consider seriously because what it means is that one of you will not be the biological parent of the child. From your mail, you mentioned artificial insemination which suggests a possible male sperm donor.
First, the person has to be AA, and secondly, the father (your husband) will have to be absolutely sure that he is ready to accept the baby as his. Also, the donor would have to understand and possibly sign an undertaking that he has no claim to the child after the procedure in the future.
It would be worth having a serious discussion on these angles and possibly seek the opinion of a professional counsellor.
Another option available is adoption which is available in Ghana for you to explore. Irrespective of these options, the choice still remains yours to consider as a couple.
Comments are closed.